
Ritalin

With thanks to Ann Wills for sending me this link.
On seeing this article I was reminded of a case brought to me in 1990. A mother brought in her 12 year-old son, claiming he had ADHD. Somewhat bewildered, this little boy sat quietly beside her while she asked what could be done for his condition.
The problem was, I couldn’t see any condition. Nothing that she told me about her son sounded at all abnormal. I explained that a child with ADHD cannot sit still in a chair, and, at worst, would be trying to lift the filing cabinets and fling them around the room.
I’m not at all sure she was willing to believe me, and I felt very sorry indeed for her son, who was being made to feel there was something wrong with him when there wasn’t. But I did give his mother good health advice for the family, especially keeping sugar to a minimum and avoiding food colourings, which are known to over-stimulate many children. Who knows what harm vaccines also do to children’s brains besides causing autism in so many.
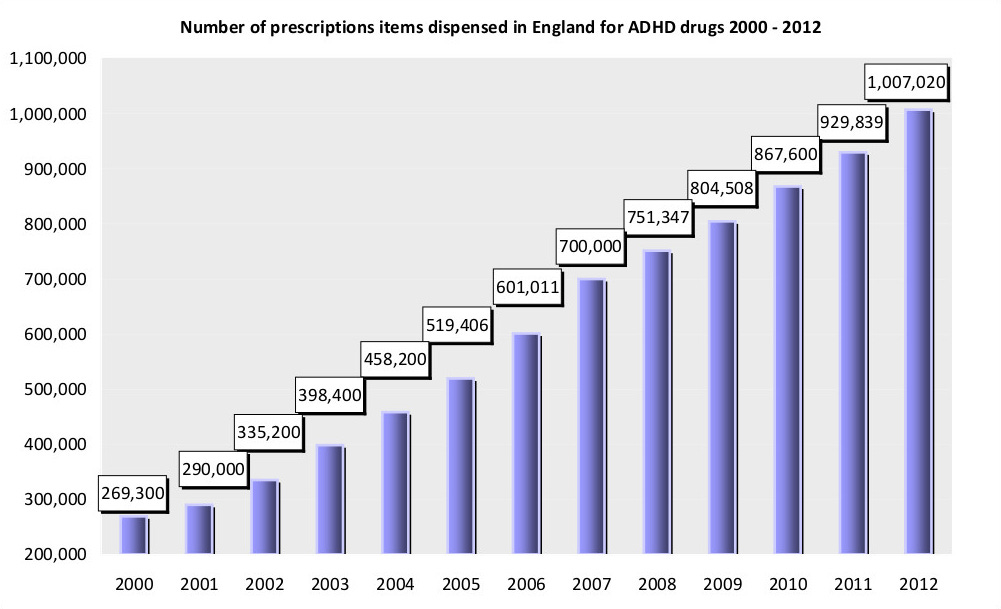
Not long after 1990, anti-ADHD drugs exploded on the scene, and prescriptions for children were given out like sweets. Many of us working in natural medicine believed that the well-publicised studies using a dietary approach to treat ADHD1 ,2 were the trigger for the development of these drugs. The drug companies knew parents and doctors were much more likely to approve of a pill rather than all the inconvenience of dietary adjustments. And look how right they were.
They also made sure everyone knew about the indications for prescribing this drug so that the discerning parent could rush their child to the doctor if any of the following signs appeared.
I’m sure food additive manufacturers and the sugar industry breathed a sigh of relief.
Egger and colleagues at the Institute of Child Health, London, gave 72 hyperactive children a hypoallergenic diet (low in foods likely to cause allergic reactions). 62 improved and 21 of these achieved normal behaviour. 28 of the children were then given foods previously excluded. Hyperactivity symptoms returned much more frequently in these children than in others given a placebo (inert substance). Artificial colourings and preservatives provoked reactions most frequently, but no child was sensitive to these alone. Controlled trial of oligoantigenic treatment in the hyperkinetic syndrome. The Lancet, March 9, 1985.
The National Society for Research into Allergy (UK), working with Superintendent Peter Bennett of the West Yorkshire Police, carried out a study on ten random habitual young offenders with an average age of 11 years. Most were destined for institutional care. On psychological testing, every child was found to be hyperactive. On nutritional testing, all the children were found to be very low in zinc. Some also had manganese and chromium deficiencies.
The children were given a diagnostic diet, low in all the foods which allergic people most commonly react to. Foods were then reintroduced one by one into the diet to see if a relapse would occur. If it did, that food was then excluded permanently.
All the eight children who finished the programme responded to the diet with a dramatic reduction in their behavioural problems. Six months later, five of the children still remained free of problems. At the same time, the rates of shoplifting, car theft and criminal damage in Shipley dropped by up to 50 per cent. This was thought to be because these five children (who lived in Shipley) had been responsible for a large proportion of these local crime statistics. Nat Soc for Research into Allergy. The Shipley Project, West Yorks, 1992.
There were several more studies, these two are just a sample.